Parathyroid Disorders Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Parathyroid Disorders. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Parathyroid Disorders Indian Medical PG Question 1: In hypoparathyroidism:
- A. Plasma calcium is high and inorganic phosphorous low
- B. Plasma calcium and inorganic phosphorous are low
- C. Plasma calcium is low and inorganic phosphorous high (Correct Answer)
- D. Plasma calcium and inorganic phosphorous are high
Parathyroid Disorders Explanation: ***Plasma calcium is low and inorganic phosphorous high***
- **Hypoparathyroidism** is characterized by insufficient parathyroid hormone (PTH) production, leading to decreased bone resorption and reduced renal reabsorption of calcium [1]. This results in **hypocalcemia** (low plasma calcium) [1].
- PTH also promotes renal excretion of phosphate [2]. With insufficient PTH, renal phosphate excretion is impaired, leading to **hyperphosphatemia** (high inorganic phosphorus) [1].
*Plasma calcium is high and inorganic phosphorous low*
- This profile is characteristic of **primary hyperparathyroidism**, where excessive PTH causes increased bone resorption and renal calcium reabsorption (high calcium), and increased renal phosphate excretion (low phosphorus).
- It directly contradicts the defining features of hypoparathyroidism [1].
*Plasma calcium and inorganic phosphorous are low*
- While plasma calcium is low in hypoparathyroidism, plasma inorganic phosphorus is characteristically high, not low [1].
- A combination of low calcium and low phosphorus can be seen in conditions like **vitamin D deficiency** (osteomalacia), but not directly in pure hypoparathyroidism [1].
*Plasma calcium and inorganic phosphorous are high*
- This combination of high calcium and high phosphorus is uncommon and not typically seen in either hypoparathyroidism or hyperparathyroidism.
- It could potentially indicate conditions like **milk-alkali syndrome** or **vitamin D intoxication**, but not hypoparathyroidism, which is defined by low calcium [1].
Parathyroid Disorders Indian Medical PG Question 2: The most common cause of severe hypercalcemia is
- A. Malignancy (Correct Answer)
- B. Vitamin D toxicity
- C. Sarcoidosis
- D. Chronic renal failure
Parathyroid Disorders Explanation: ***Malignancy***
- **Malignancy** is the most frequent cause of **severe hypercalcemia**, often resulting from **parathyroid hormone-related peptide (PTHrP) secretion** (humoral hypercalcemia of malignancy) or **bone metastases** causing osteolysis [1].
- Cancers like **squamous cell carcinoma**, **breast cancer**, **multiple myeloma**, and **renal cell carcinoma** are commonly associated with severe hypercalcemia [1].
*Vitamin D toxicity*
- While vitamin D toxicity can cause hypercalcemia, it typically leads to **moderate hypercalcemia** and is less common as a cause of **severe hypercalcemia** compared to malignancy [1].
- It usually occurs due to **excessive intake of vitamin D supplements** or activated vitamin D [1].
*Sarcoidosis*
- Sarcoidosis can cause hypercalcemia due to **extrarenal production of 1,25-dihydroxyvitamin D** by activated macrophages [1].
- However, the hypercalcemia in sarcoidosis is usually **mild to moderate** and rarely reaches the severity seen with malignancy [1].
*Chronic renal failure*
- **Chronic renal failure** is more commonly associated with **hypocalcemia** due to impaired vitamin D activation and hyperparathyroidism [2], [3].
- While some patients with end-stage renal disease and **adynamic bone disease** or **tertiary hyperparathyroidism** can develop hypercalcemia, it is not the most common cause of *severe* hypercalcemia in the general population.
Parathyroid Disorders Indian Medical PG Question 3: Secondary hyperparathyroidism due to Vit D deficiency shows :
- A. Hypocalcemia (Correct Answer)
- B. Hypophosphatemia
- C. Hypercalcemia
- D. Hyperphosphatemia
Parathyroid Disorders Explanation: ***Hypocalcemia***
- **Vitamin D deficiency** leads to decreased intestinal absorption of calcium, causing **hypocalcemia** [3].
- This persistent **low serum calcium** is the primary stimulus for the parathyroid glands to increase PTH secretion, leading to secondary hyperparathyroidism [1], [2].
*Hypophosphatemia*
- While PTH typically promotes phosphate excretion in the kidneys leading to hypophosphatemia, in **secondary hyperparathyroidism due to vitamin D deficiency**, the effect on phosphate can be variable [3].
- The goal of increased PTH is to raise calcium, and maintaining some level of phosphate is necessary for bone health and proper calcium regulation. Early or mild deficiency may not show significant hypophosphatemia.
*Hypercalcemia*
- **Hypercalcemia** is a characteristic feature of **primary hyperparathyroidism**, where the parathyroid glands autonomously overproduce PTH [1].
- In secondary hyperparathyroidism (due to vitamin D deficiency), the PTH is elevated in response to **low calcium**, and sustained significant hypercalcemia is not expected; in fact, the underlying problem is **hypocalcemia** [1].
*Hyperphosphatemia*
- **PTH** generally acts to lower serum phosphate levels by promoting its renal excretion [2].
- Therefore, **hyperphosphatemia** is not typically observed in secondary hyperparathyroidism; rather, a more common finding would be normal or low phosphate due to the elevated PTH [3].
Parathyroid Disorders Indian Medical PG Question 4: In a patient with parathyroid adenoma, how do we confirm the removal of the correct gland after surgery?
- A. 50% reduction in PTH after 10 minutes (Correct Answer)
- B. 25% reduction in PTH after 10 minutes
- C. 25% reduction in PTH after 5 minutes
- D. 50% reduction in PTH after 5 minutes
Parathyroid Disorders Explanation: ***50% reduction in PTH after 10 minutes***
- Intraoperative **PTH monitoring** is crucial for confirming complete removal of hyperfunctioning parathyroid tissue during parathyroidectomy.
- A successful surgery is indicated by a **≥50% drop** in PTH levels from the baseline (pre-excision) or highest post-excision level within **10 minutes** of gland removal.
*25% reduction in PTH after 10 minutes*
- A **25% reduction** in PTH after 10 minutes is generally considered **insufficient** to confirm successful removal of the hyperfunctioning gland.
- This level of reduction may suggest incomplete removal or the presence of additional hypersecreting tissue.
*25% reduction in PTH after 5 minutes*
- While an initial drop may be observed, a **25% reduction after only 5 minutes** without further significant decline by 10 minutes is often not indicative of successful surgery.
- The standard MIBI-scan-guided protocol or the Miami criteria require a more substantial and sustained drop.
*50% reduction in PTH after 5 minutes*
- A rapid and significant **50% reduction after 5 minutes** of excision is a good sign but the gold standard for intraoperative PTH monitoring typically requires the **10-minute post-excision** sample to confirm the sustained drop.
- The **Miami Criteria**, a widely accepted protocol, uses the 10-minute post-excision time point as a critical determinant.
Parathyroid Disorders Indian Medical PG Question 5: A patient develops recurrent hyperparathyroidism 2 years after initial parathyroidectomy and has experienced cardiovascular complications due to persistent hypercalcemia. What is the most appropriate management?
- A. Repeat neck surgery
- B. Observation and repeat serum Ca2+ in two months
- C. Repeat parathyroidectomy after medical optimization (Correct Answer)
- D. Medical management with calcimimetics (cinacalcet)
Parathyroid Disorders Explanation: ***Repeat parathyroidectomy after medical optimization***
- Recurrent **hyperparathyroidism** often requires repeat surgery, particularly in patients who have experienced cardiovascular events, as persistent hypercalcemia can exacerbate cardiac risk.
- **Medical optimization** of cardiovascular conditions and metabolic status before reoperation is crucial to minimize surgical risks and improve outcomes.
*Repeat neck surgery*
- While repeat neck surgery is often necessary, this option is incomplete as it does not sufficiently emphasize the importance of **medical optimization** in patients with a history of cardiovascular events.
- Performing surgery without adequate pre-operative evaluation and optimization can lead to increased **perioperative complications** in this high-risk group.
*Observation and repeat serum Ca2+ in two months*
- **Observation** is generally not appropriate for recurrent hyperparathyroidism, especially when it has already led to cardiovascular events, as continued hypercalcemia poses significant long-term health risks.
- Delaying definitive treatment allows for ongoing end-organ damage, including worsening **cardiovascular disease** and bone complications.
*Medical management with calcimimetics (cinacalcet)*
- **Calcimimetics** like **cinacalcet** can reduce parathyroid hormone (PTH) and calcium levels, but they are typically used as an adjunct or for patients who are not surgical candidates.
- In cases of recurrent hyperparathyroidism, especially with clinical sequelae like cardiovascular events, **surgical removal of the adenoma** remains the definitive treatment to achieve a cure.
Parathyroid Disorders Indian Medical PG Question 6: What is the investigation of choice for detecting recurrence after parathyroid gland surgery?
- A. SPECT
- B. MRI
- C. Neck ultrasound
- D. Sestamibi scan (Correct Answer)
Parathyroid Disorders Explanation: ***Sestamibi scan***
- A **sestamibi scan** is the investigation of choice for **localizing recurrent or persistent hyperparathyroidism** because **parathyroid tissue preferentially retains the tracer** longer than thyroid tissue.
- This nuclear medicine imaging technique helps identify ectopic or very small parathyroid adenomas, which may be difficult to locate with other methods.
*SPECT*
- **Single-photon emission computed tomography (SPECT)** can be used as an adjunct to a sestamibi scan (SPECT-Sestamibi) to provide 3D images and improve localization, but it is typically not the initial or standalone investigation of choice for recurrence.
- While SPECT offers increased sensitivity and specificity over planar imaging by removing superimposed structures, the **sestamibi uptake itself is the crucial diagnostic marker**.
*MRI*
- **Magnetic resonance imaging (MRI)** is generally used for detailed anatomical assessment of the neck and mediastinum, especially if there's concern for **ectopic glands or complex anatomy**.
- However, it is less sensitive than sestamibi for detecting small or recurrent hyperactive parathyroid tissue due to its reliance on anatomical rather than functional abnormalities.
*Neck ultrasound*
- **Neck ultrasound** is an excellent initial imaging modality for primary hyperparathyroidism due to its **affordability and ability to visualize cervical parathyroid glands**.
- For detecting recurrence, its utility is limited, especially in cases of **ectopic glands** (e.g., in the mediastinum) or if scar tissue hinders clear visualization.
Parathyroid Disorders Indian Medical PG Question 7: A patient is on a low calcium diet for 8 weeks. Which of the following increases to maintain serum calcium levels?
- A. Active 24,25 dihydroxy cholecalciferol
- B. PTH (Correct Answer)
- C. Serum phosphate level
- D. Calcitonin
Parathyroid Disorders Explanation: ***PTH***
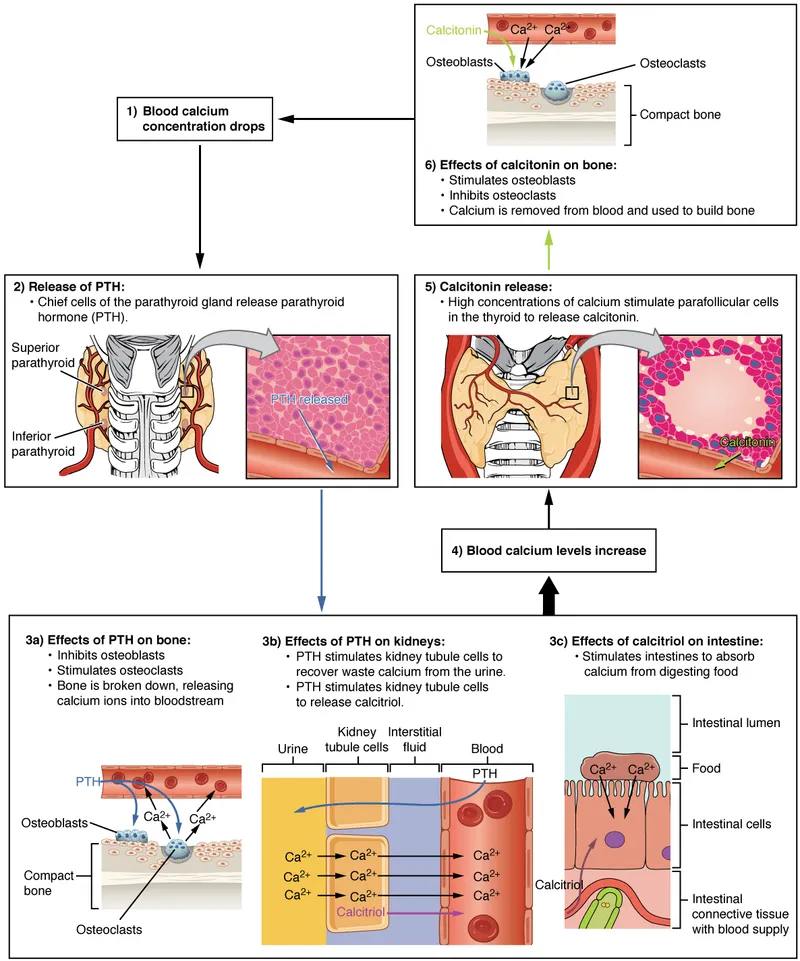
- **Parathyroid hormone (PTH)** is the primary regulator of calcium homeostasis and the key hormone that **increases in response to hypocalcemia** (low serum calcium).
- In a patient on a low calcium diet for 8 weeks, **PTH secretion increases** to maintain normal serum calcium levels.
- PTH acts through three main mechanisms: increasing **bone resorption** (releasing calcium from bone), enhancing renal **calcium reabsorption** in the distal tubule, and stimulating the production of **active vitamin D (1,25-dihydroxycholecalciferol)** which increases intestinal calcium absorption.
*Active 24,25 dihydroxy cholecalciferol*
- **24,25-dihydroxycholecalciferol** is a relatively **inactive metabolite** of vitamin D and represents a pathway of vitamin D catabolism, not activation.
- The **active form** of vitamin D that increases calcium absorption is **1,25-dihydroxycholecalciferol (calcitriol)**, whose production is stimulated by PTH.
- This metabolite does **not increase** in response to hypocalcemia as a compensatory mechanism.
*Serum phosphate level*
- A low calcium diet would **not directly lead to an increase in serum phosphate levels**.
- In fact, PTH (which increases in response to low calcium) typically causes a **decrease in serum phosphate** by promoting renal phosphate excretion (phosphaturic effect).
- High phosphate levels can actually exacerbate hypocalcemia by forming insoluble calcium-phosphate complexes.
*Calcitonin*
- **Calcitonin** is released from the thyroid parafollicular cells (C cells) in response to **high serum calcium levels** (hypercalcemia).
- It acts to **lower** calcium by inhibiting osteoclast activity and reducing renal calcium reabsorption.
- In hypocalcemia (low calcium diet), calcitonin secretion would **decrease, not increase**, making this the opposite of what occurs to maintain calcium homeostasis.
Parathyroid Disorders Indian Medical PG Question 8: Hypocalcemia is characterized by all except
- A. Carpopedal spasm
- B. Hyperactive tendon reflexes
- C. Numbness and tingling of circumoral region
- D. Shortening of Q-T interval in ECG (Correct Answer)
Parathyroid Disorders Explanation: ***Shortening of Q-T interval in ECG***
- Hypocalcemia typically causes **prolongation of the QT interval** on an ECG due to delayed repolarization of ventricular myocardial cells.
- A **shortened QT interval** is usually associated with hypercalcemia or conditions like short QT syndrome.
*Carpopedal spasm*
- This is a classic sign of hypocalcemia, known as **Trousseau's sign**, elicited by inflating a blood pressure cuff above systolic pressure, which causes spasm of the hand and foot.
- It results from increased neuromuscular irritability due to lower calcium levels.
*Hyperactive tendon reflexes*
- Hypocalcemia leads to **increased neuromuscular excitability**, which manifests as hyperactive or brisk deep tendon reflexes.
- This heightened reflex activity is a common neurological symptom of low calcium.
*Numbness and tingling of circumoral region*
- This symptom, known as **paresthesia**, is a very common and early manifestation of hypocalcemia.
- It occurs due to the increased excitability of peripheral nerves caused by reduced extracellular calcium.
Parathyroid Disorders Indian Medical PG Question 9: Secondaries in the neck with no obvious primary malignancy is most often due to which of the following?
- A. Carcinoma of the Stomach
- B. Carcinoma of the Larynx
- C. Carcinoma of the Nasopharynx (Correct Answer)
- D. Carcinoma of the Thyroid
Parathyroid Disorders Explanation: **Explanation:**
The clinical scenario of "Secondary in the neck with an unknown primary" refers to a metastatic cervical lymph node where the initial site of malignancy is not clinically apparent.
**Why Nasopharynx is the correct answer:**
Carcinoma of the Nasopharynx is notorious for being "clinically silent" in its early stages. Due to its anatomical location in the fossa of Rosenmüller, the primary tumor often remains small and asymptomatic while early lymphatic spread occurs. In approximately **50-60% of cases**, a painless neck swelling (usually involving the upper deep cervical or Level V nodes) is the first and only presenting symptom. This makes it the most common site for an occult primary in the head and neck region.
**Analysis of Incorrect Options:**
* **Carcinoma of the Stomach:** While it can metastasize to the left supraclavicular node (Virchow’s node/Troisier’s sign), it is a distant metastasis (Stage IV) and usually presents with significant constitutional or GI symptoms.
* **Carcinoma of the Larynx:** These tumors typically present early with symptoms like hoarseness of voice (glottic) or throat pain/dysphagia (supraglottic), making the primary site "obvious" rather than occult.
* **Carcinoma of the Thyroid:** While it frequently spreads to cervical nodes (especially papillary variety), the primary thyroid nodule is usually palpable or easily detected on initial physical examination.
**High-Yield Clinical Pearls for NEET-PG:**
* **Most common site of occult primary:** Nasopharynx (followed by Palatine Tonsil and Base of Tongue).
* **Diagnostic Gold Standard:** Fine Needle Aspiration Cytology (FNAC) is the first-line investigation for the neck mass.
* **Work-up:** If the primary is not found on physical exam, the next steps include **CECT/MRI** from skull base to clavicle and **Panendoscopy** (Direct laryngoscopy, Esophagoscopy, and Bronchoscopy) with guided biopsies.
* **EBV Association:** Nasopharyngeal carcinoma is strongly associated with the Epstein-Barr Virus.
Parathyroid Disorders Indian Medical PG Question 10: What clinical appearance is associated with bilateral TMJ ankylosis?
- A. Bird face appearance
- B. Vogel gesicht appearance
- C. Andy gump appearance
- D. All of the above (Correct Answer)
Parathyroid Disorders Explanation: **Explanation:**
Bilateral Temporomandibular Joint (TMJ) ankylosis, especially when it occurs during the developmental years, leads to a characteristic facial deformity due to the failure of mandibular growth.
**1. Why "All of the above" is correct:**
The terms **Bird face appearance**, **Vogel gesicht appearance**, and **Andy Gump appearance** are all synonymous in clinical ENT and Maxillofacial surgery to describe the same morphological profile.
* **Bird face / Vogel gesicht:** "Vogel gesicht" is simply the German translation for "Bird face." It describes the profile where the mandible is severely retruded (micrognathia/retrognathia), making the nose appear prominent and the face resemble a bird.
* **Andy Gump appearance:** Named after a famous 1920s comic strip character, this term refers to the severe receding chin (retrognathia) seen in these patients.
**2. Pathophysiology:**
The mandibular condyle is the primary growth center of the mandible. Bilateral ankylosis results in the cessation of forward and downward growth of the lower jaw. This leads to:
* Micrognathia (small jaw) and Retrognathia (receded jaw).
* Secondary features like "Antegonial notching" and a double chin appearance.
**3. High-Yield Clinical Pearls for NEET-PG:**
* **Unilateral Ankylosis:** Results in facial asymmetry with the chin deviating **towards** the affected side.
* **Bilateral Ankylosis:** Results in symmetrical recession (Bird face) without deviation.
* **Most common cause:** Trauma (especially birth trauma or falls on the chin) followed by infections (Otitis media).
* **Treatment:** Gap arthroplasty or Interpositional arthroplasty. Early surgery is crucial to prevent permanent growth restriction.
* **Airway Concern:** These patients are difficult to intubate (Difficult Airway) due to limited mouth opening and retrognathia.
More Parathyroid Disorders Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.