Laryngomalacia Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Laryngomalacia. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Laryngomalacia Indian Medical PG Question 1: 2 months old child having birth weight 2kg, with poor feeding, very sleepy and wheezing. The diagnosis is?
- A. Very severe disease (Correct Answer)
- B. No evidence of pneumonia
- C. Severe respiratory infection
- D. No diagnosis
Laryngomalacia Explanation: ***Very severe disease***
- According to **WHO/IMNCI (Integrated Management of Neonatal and Childhood Illness) classification** for young infants (0-2 months), the presence of **danger signs** automatically classifies the condition as "Very severe disease"
- This infant presents with two critical danger signs: **poor feeding** and **lethargy (very sleepy)**, along with respiratory symptoms (wheezing)
- In young infants, any danger sign (poor feeding, lethargic/unconscious, convulsions, severe chest indrawing, central cyanosis) requires immediate classification as "Very severe disease" and **urgent referral** to higher center
- This is a specific diagnostic classification used in pediatric emergency protocols, not a general term
*Severe respiratory infection*
- While the child has respiratory symptoms (wheezing), this classification would only be appropriate if respiratory distress was present **without danger signs**
- The presence of danger signs (poor feeding, lethargy) escalates the classification to "Very severe disease" in the WHO/IMNCI protocol
- In young infants (0-2 months), the classification system prioritizes danger signs over organ-specific diagnoses
*No evidence of pneumonia*
- This is incorrect as the infant clearly presents with respiratory symptoms (wheezing) and systemic signs of illness
- The presence of wheezing, poor feeding, and lethargy indicates serious illness requiring urgent evaluation and treatment
- This option contradicts the clinical presentation
*No diagnosis*
- This is incorrect as the WHO/IMNCI classification provides a clear diagnostic framework
- The presence of danger signs in a young infant mandates classification as "Very severe disease"
- A working diagnosis is essential for guiding appropriate management and urgent referral
Laryngomalacia Indian Medical PG Question 2: Most common cause of intermittent stridor in a 10-day-old child shortly after birth is:
- A. Hypertrophy of turbinate
- B. Laryngomalacia (Correct Answer)
- C. Foreign body
- D. Vocal nodule
Laryngomalacia Explanation: ***Laryngomalacia***
- This is the **most common cause** of congenital stridor, typically becoming noticeable within the first few weeks of life, consistent with a 10-day-old child.
- The stridor is characteristically **intermittent**, worsens with crying or feeding, and improves when prone, due to the collapse of supraglottic structures.
*Hypertrophy of turbinate*
- While nasal issues can cause **stertor** (a snoring sound), hypertrophy of turbinates is not a common cause of stridor in an infant.
- **Stridor** originates from the larynx or trachea, not the nasal passages.
*Foreign body*
- An aspirated foreign body would typically cause **acute-onset stridor** that is often continuous and associated with choking or coughing spells, rather than intermittent symptoms starting shortly after birth.
- This is a less likely etiology for intermittent stridor developing within the first two weeks of life.
*Vocal nodule*
- Vocal nodules are generally associated with **hoarseness** or a change in voice quality, and typically require chronic vocal abuse to develop.
- They are exceptionally rare in neonates and would not present as intermittent stridor.
Laryngomalacia Indian Medical PG Question 3: Which of the following conditions is treated by laser-assisted uvulopalatoplasty?
- A. Stammering
- B. Pharyngotonsillitis
- C. Snoring (Correct Answer)
- D. Cleft palate
Laryngomalacia Explanation: ***Snoring***
- **Laser-assisted uvulopalatoplasty (LAUP)** is a surgical procedure used to **reduce or eliminate snoring** by reshaping the uvula and soft palate.
- This procedure helps to open the airway by removing excess tissue, thereby reducing vibrations that cause snoring.
*Stammering*
- Stammering, or stuttering, is a **speech disorder** characterized by repetitions or prolongations of sounds, syllables, or words.
- Its treatment typically involves **speech therapy** and behavioral interventions, not surgical procedures like LAUP.
*Pharyngotonsillitis*
- Pharyngotonsillitis is an inflammation of the **pharynx and tonsils**, commonly caused by bacterial or viral infections.
- Treatment usually involves **antibiotics** for bacterial infections or supportive care for viral infections, and in severe recurrent cases, a **tonsillectomy** may be performed, not LAUP.
*Cleft palate*
- A cleft palate is a birth defect where the roof of the mouth does not form completely, resulting in an **opening that can extend to the nasal cavity**.
- Its treatment involves **reconstructive surgery** to close the opening, often performed in infancy, which is distinct from LAUP.
Laryngomalacia Indian Medical PG Question 4: Which of the following statements about the upper airways of a neonate is true?
- A. The larynx extends from C1 to C3.
- B. The epiglottis is large and omega-shaped. (Correct Answer)
- C. More than one of the above statements is true.
- D. The cricoid cartilage is the narrowest part of the airway in neonates.
Laryngomalacia Explanation: ***The epiglottis is large and omega-shaped.***
- In neonates, the **epiglottis** is relatively **large**, U-shaped or **omega-shaped**, and floppy
- This anatomical feature can contribute to airway obstruction due to its proximity to the soft palate
- This anatomical difference from adults has important implications for **intubation and airway management**, as it makes visualizing the vocal cords more challenging
- **This is the correct statement** about neonatal upper airway anatomy
*The larynx extends from C1 to C3.*
- The **larynx of a neonate** is located more **superiorly** and anteriorly compared to an adult, generally extending from **C3 to C4** (NOT C1 to C3)
- Its higher position contributes to the neonate's obligate **nasal breathing** and makes the airway more susceptible to obstruction
- The stated vertebral level (C1-C3) is **incorrect**
*The cricoid cartilage is the narrowest part of the airway in neonates.*
- **Historically**, the **cricoid cartilage** was considered the narrowest part of the pediatric airway, and this remains in many older textbooks
- **Recent evidence** suggests that the **rima glottidis** (at the level of the vocal cords) is actually the narrowest point in most neonates and children
- This evolving understanding has implications for **tube sizing** and airway management in pediatric patients
- Based on current anatomical evidence, this statement is considered **incorrect**
*More than one of the above statements is true.*
- As only **one statement** is anatomically correct regarding the neonate's upper airway (the omega-shaped epiglottis), this option is **incorrect**
- The detailed anatomical differences, such as the position of the larynx and the shape of the epiglottis, are crucial for understanding neonatal airway physiology
Laryngomalacia Indian Medical PG Question 5: Esophageal manometry was performed - it revealed panesophageal pressurization with distal contractile integrity as >450mm Hg pressure in the body. What will be the diagnosis?
- A. Type 2 achalasia
- B. Type 3 achalasia (Correct Answer)
- C. Jackhammer esophagus
- D. Type 1 achalasia (classic achalasia)
Laryngomalacia Explanation: The diagnosis is Type 3 achalasia. This condition is characterized by panesophageal pressurization, indicating diffuse, simultaneous contractions throughout the esophagus. The high distal contractile integrity (>450 mmHg pressure) further supports Type 3 achalasia, which involves significant spastic contractions. In contrast, while high-resolution manometry allows for the accurate classification of these motility abnormalities [1], other types present differently. Type 1 achalasia (classic achalasia) is marked by failed esophageal peristalsis and absent or minimal esophageal pressurization [1]. The primary characteristic is incomplete or absent lower esophageal sphincter (LES) relaxation, not hypercontractility [1]. Type 2 achalasia is identified by esophageal panesophageal pressurization (simultaneous contractions), but with normal to high contractile pressures, not the extremely high values seen here. Jackhammer esophagus involves hypercontractility (distal contractile integral >8000 mmHg·cm·s) and is characterized by rapid, repetitive, and fragmented contractions, rather than the diffuse panesophageal pressurization and spasticity typical of Type 3 achalasia [2].
Laryngomalacia Indian Medical PG Question 6: Which of the following statements about laryngomalacia is true?
- A. It is characterized by an omega-shaped epiglottis.
- B. It requires immediate surgical intervention.
- C. It always requires surgical intervention in newborns.
- D. It typically presents with inspiratory stridor. (Correct Answer)
Laryngomalacia Explanation: ***It typically presents with inspiratory stridor.***
- **Laryngomalacia** is the most common cause of **inspiratory stridor** in infants, usually presenting within the first few weeks of life due to collapse of supraglottic structures during inspiration.
- The stridor is characteristically **worse when crying, feeding, or lying supine**, and often improves when the infant is prone.
*It is characterized by an omega-shaped epiglottis.*
- While an **omega-shaped epiglottis** can be a feature seen in laryngomalacia, it is not the sole or defining characteristic and is not universally present.
- The primary characteristic is the **collapse of the supraglottic structures** (arytenoids, aryepiglottic folds, and epiglottis) into the laryngeal inlet upon inspiration.
*It requires immediate surgical intervention.*
- The vast majority of **laryngomalacia cases are mild to moderate** and resolve spontaneously by 12-18 months of age, requiring only conservative management.
- **Surgical intervention** (supraglottoplasty) is reserved for severe cases with significant feeding difficulties, failure to thrive, severe airway obstruction, or apneic episodes.
*It always requires surgical intervention in newborns.*
- As mentioned, **most cases are self-limiting** and do not require surgery, especially in newborns.
- Surgical intervention is only considered when there are **severe symptoms** impacting the infant's health and development.
Laryngomalacia Indian Medical PG Question 7: Laser uvulopalatoplasty is indicated for which of the following conditions?
- A. Obstructive sleep apnea (Correct Answer)
- B. Pharyngotonsillitis
- C. Cleft palate
- D. Stammering
Laryngomalacia Explanation: ***Obstructive sleep apnea***
- **Laser uvulopalatoplasty (LUP)** is a surgical procedure that reshapes the **uvula** and **soft palate** to enlarge the airway in patients with **obstructive sleep apnea (OSA)**.
- OSA is characterized by repetitive episodes of upper airway obstruction during sleep, leading to snoring, daytime sleepiness, and other health issues.
*Pharyngotonsillitis*
- This condition involves inflammation of the **pharynx** and **tonsils**, usually caused by bacterial or viral infections.
- Treatment typically involves antibiotics for bacterial infections or symptomatic relief for viral infections, not surgical reshaping of the palate.
*Cleft palate*
- **Cleft palate** is a congenital birth defect where the roof of the mouth does not fully close during fetal development.
- The primary treatment involves **surgical repair** to close the opening, which is a different procedure from LUP and focuses on reconstructing normal anatomy.
*Stammering*
- **Stammering** is a **speech disorder** characterized by disruptions in fluency, such as repetitions, prolongations, or blocks in speech.
- It is managed through **speech therapy** and behavioral interventions, and is unrelated to airway obstruction or surgical procedures on the palate.
Laryngomalacia Indian Medical PG Question 8: A child presents with high grade fever, inspiratory stridor and develops swallowing difficulty with drooling of saliva since last 4-6 hours. Which of the following treatment is recommended apart from general airway management?
- A. IV ceftriaxone (Correct Answer)
- B. Anti-diphtheria toxin
- C. Corticosteroids
- D. Nebulized racemic epinephrine
Laryngomalacia Explanation: ***IV ceftriaxone***
- The symptoms (high-grade fever, inspiratory stridor, swallowing difficulty with drooling, rapid onset) are highly suggestive of **acute epiglottitis**, a life-threatening emergency.
- **Empiric intravenous antibiotics** like ceftriaxone are crucial for treating the bacterial infection (commonly *Haemophilus influenzae* type b or *Streptococcus pneumoniae*) causing epiglottitis.
*Anti-diphtheria toxin*
- This treatment is specific for **diphtheria**, which causes a pseudomembrane and can lead to airway obstruction, but the clinical picture here is more consistent with epiglottitis due to its rapid and severe presentation without mention of a pseudomembrane.
- Diphtheria typically has a more gradual onset and is characterized by a **grayish pseudomembrane** in the throat, unmentioned in this case.
*Corticosteroids*
- While corticosteroids are used in other forms of upper airway obstruction (like **croup**), their role in acute epiglottitis is controversial and not a primary life-saving measure; antibiotics and airway management are paramount.
- Their primary benefit lies in reducing inflammation, but they do not address the acute bacterial cause of epiglottitis directly and are secondary to antibiotics.
*Nebulized racemic epinephrine*
- This treatment is primarily used for **laryngotracheobronchitis (croup)**, which presents with a barking cough and stridor, but typically lacks the high fever and severe drooling seen in epiglottitis.
- Nebulized racemic epinephrine helps to reduce subglottic edema in croup but would not be effective against the severe supraglottic swelling of epiglottitis, nor would it treat the underlying bacterial infection.
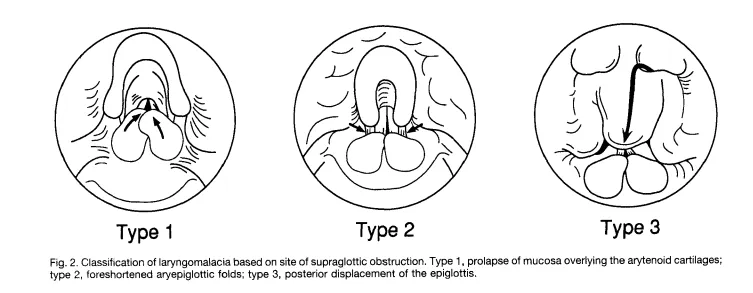
Laryngomalacia Indian Medical PG Question 9: All of the following are correct about the image shown except:
- A. Omega shaped epiglottis
- B. High pitched expiratory stridor (Correct Answer)
- C. Cry is normal
- D. 10% cases need surgery due to development of OSA or Cor Pulmonale
Laryngomalacia Explanation: ***High pitched expiratory stridor***
- The image depicts an **omega-shaped epiglottis** and collapsed aryepiglottic folds, consistent with **laryngomalacia**.
- Laryngomalacia typically presents with **inspiratory stridor**, not expiratory, resulting from airway collapse during inspiration.
- **This is the EXCEPT answer** - high-pitched expiratory stridor is NOT a feature of laryngomalacia.
*Omega shaped epiglottis*
- The image clearly shows an **omega-shaped epiglottis**, a characteristic feature of **laryngomalacia**.
- This anatomical variation contributes to the collapse of supraglottic structures during inspiration.
*Cry is normal*
- In laryngomalacia, the **vocal cords** themselves are not affected, so the **cry typically remains normal**.
- The abnormal sounds (stridor) arise from the supraglottic structures, not the vocal cord function during crying.
*10% cases need surgery due to development of OSA or Cor Pulmonale*
- While most cases of laryngomalacia are self-limiting, approximately **10% of infants may require surgical intervention** (supraglottoplasty).
- This is usually due to severe symptoms like **obstructive sleep apnea (OSA)**, failure to thrive, or the rare development of **cor pulmonale**.
Laryngomalacia Indian Medical PG Question 10: All of the following statements about laryngomalacia are true, except for:
- A. It is associated with an omega shaped epiglottis
- B. Surgical Tracheostomy is the treatment of choice (Correct Answer)
- C. It is the most common congenital anomaly of the larynx
- D. Stridor is increased on crying and relieved on lying prone
Laryngomalacia Explanation: ***Surgical Tracheostomy is the treatment of choice***
- While laryngomalacia is the most common cause of **stridor** in infants, most cases are **mild and self-limiting**, resolving spontaneously by **12 to 18 months of age**.
- **Surgical tracheostomy** is reserved for severe cases with significant **airway obstruction**, **failure to thrive**, or **life-threatening apneic spells** after failed conservative management and supraglottoplasty.
*It is the most common congenital anomaly of the larynx*
- This statement is **true**; laryngomalacia is indeed the most frequent congenital anomaly of the larynx, affecting approximately **60% of all congenital laryngeal anomalies**.
- It is the most common cause of **inspiratory stridor** in infants.
*It is associated with an omega shaped epiglottis*
- This statement is **true**; the characteristic finding in laryngomalacia is the collapse of the **supraglottic structures** during inspiration.
- This often includes a **long, curled, 'omega-shaped' epiglottis**, which contributes to the airway obstruction.
*Stridor is increased on crying and relieved on lying prone*
- This statement is **true**; the inspiratory stridor in laryngomalacia is typically **worsened by agitation, crying, feeding, or supine positioning**.
- Lying **prone** or **side-lying** positions can help relieve the stridor by allowing the supraglottic tissues to fall forward and open the airway.
More Laryngomalacia Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.